
Now that most of the dust has settled, we can assess what the recent election means for health care policy and advocacy. That sound you may have heard as the election results came in on November 6th was the collective sigh of relief from health care advocates (and millions of people with pre-existing conditions) because, at least for the next couple of years, there will be no further federal legislative attempts to take away the consumer protections and financial assistance provided by the ACA. Nor is there likely to be any chance for Congress to make deep cuts or fundamentally alter the Medicaid program. In addition, prospects for expanded coverage in the states look better now than they have in years.
At the same time, the election took a serious bite out of the population of red state Democrats in the Senate. While several Democrats won in states carried by President Trump (Brown, Tester, Manchin) there were also losses in North Dakota, Missouri, Indiana and Florida. Many have said this was a historically bad map for Democrats. However, 2020 does not look like a year in which Democrats are likely to make large gains. While there are more Republicans than Democrats up for reelection, most of them are in pretty safe seats. Indeed, several analysts have observed that, at least for the next few years, the Senate will be very challenging territory for Democrats.
What does all this have to do with health care? Basically, for the last 50 years, significant progress on expanding health insurance coverage has depended on a Democratic majority and the size of that majority matters.
Here are some key data points:
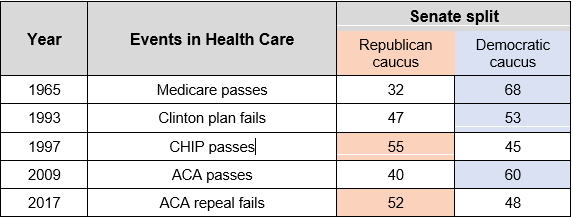
Although CHIP is a partial exception, it is an outlier. There were special considerations that led to the passage of CHIP that likely will not be repeated. In general, accomplishing big things on health care—good or bad— for either party requires a strong majority. At least for the next few years, neither party is likely to have one. On the one hand, that means no ACA repeal or fundamental restructuring of Medicaid (or Medicare); on the other hand, it means no big coverage federal expansions either.
We can expect debate and perhaps modest federal action in a number of areas, including continued work on substance use disorders, payment and delivery system reform, and prescription drug prices. One particularly encouraging development has been the growing interest on both sides of the aisle in addressing the problem of surprise out-of-network billing. But beyond those issues, there is not a lot of common ground between the parties on health care. In fact, House Republicans seem to have adopted their election post-mortem mantra from Seinfeld (no learning, no hugging). They have gone so far as to blame the loss of the House on the fact that the Senate did not pass ACA repeal. (A more rational conclusion would be that the Senators who voted against repeal, far from costing the Republicans the House, actually saved the Senate for them.)
On the other hand, federal stalemate means states still have the Medicaid funding and health care tax credits that can undergird continued advances in coverage and improved affordability. While we have to expect that the Trump administration will continue to attack key regulatory consumer protections and create new barriers to affordable coverage and care, there is substantial power to counter these measures through state law and regulation. In addition, it will be incumbent on states to look beyond coverage to advance an inclusive health policy agenda that promotes equity, quality care and better health for everyone in this diverse nation. Reversing the alarming decline in life expectancy that has hit many communities and eradicating the persistent racial disparities in health care and health that have historically plagued our country must be high on the priority list.
With thanks to Nina Oishi, program associate, for her assistance.