Getting the Health Care Cost Problem Right
There are few propositions in the health policy arena likely to command more agreement than that the United States spends too much on health care. But behind this apparent agreement, there is much less than meets the eye. It is not only that in health care, one person's waste or excess spending is another person's income. The nature and consequences of our cost problem are widely misunderstood and misrepresented in both the media and in political and policy debates. Without clarity on the nature of problem, it becomes harder to come up with the right solutions. So, in the interest of building a better understanding of exactly what is the problem we are trying to solve, here are a few common statements about health care costs that are either untrue or, at best, partly true.
Myth: Health Care takes up too much of our GDP
How many times have you heard, in the context of debate about health care costs, that health care’s growing share of our GDP is a sign of trouble? Actually, it is generally a good thing. Perhaps you are skeptical, so let’s try a simplified example:
Imagine a country with an economy that produces only two things: food and health care. And let’s say that it takes up almost all of the labor time of the workforce to grow enough food to feed people so the distribution of GDP between health care and food looks something like figure A below.
Now suppose improvements in agricultural techniques make it possible to produce all the food everyone needs with only half as much effort. Of course, they could keep all that new free time as leisure, but let’s suppose they shift to producing more health care. Now the economy looks like figure B.
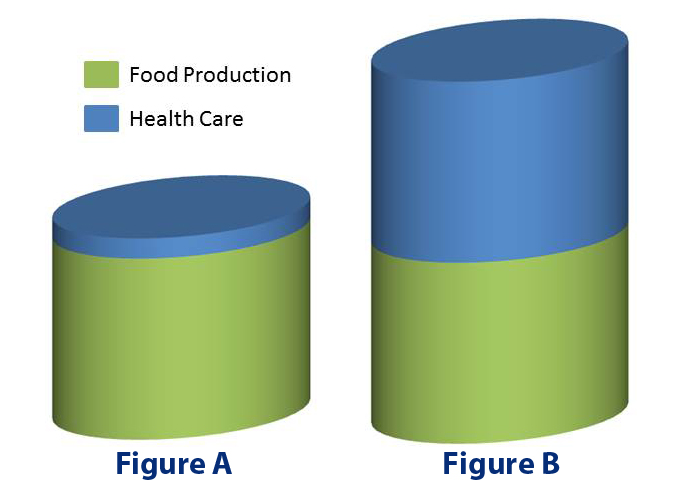
Even though health care now consumes 50% of GDP, the people are actually better off than before and certainly not in danger of having their food production crowded out by health care.
Now take a look at these two charts:
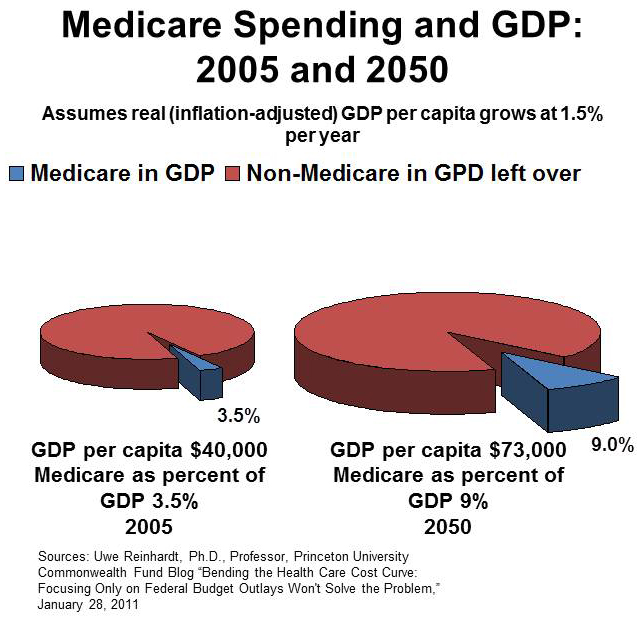
Both make essentially the same point, although one looks at Medicare spending and the other looks at health care spending as a whole. The takeaway: even if health care grows as a percent of GDP over time, we can still afford the other things we need and want.
Myth: Health care costs are hurting business and undermining our international competitiveness
The claim that high and rising health care costs undermine our international competitiveness is frequently made by some employers, particularly manufacturers. However, economic theory and the available empirical evidence cast doubt on this claim. Research shows that employer health care spending is almost entirely an offset against wages. Not only that, but the share of GDP going to total compensation (wages plus benefits) has been stagnant or falling for the past 40 years even as health care has claimed an ever larger share of our GDP. If total compensation was rising along with rising health care spending, you could argue for a connection. But with compensation flat or falling, it is hard to make the case.
Myth: Rising health care costs, particularly Medicare and Medicaid, are crowding our ability to afford other things we need like education and infrastructure.
OK, maybe this one is half true. Rising health care costs need not crowd out our ability to afford education or other social welfare spending any time soon (or maybe ever), although they may force us to reexamine other policies and commitments. For example, our level of military spending exceeds the levels of the next eight highest spending countries combined. Our incarceration rate—the highest in the world and more than double the rate in 1980—costs our state and local governments billions. At the same time we incur these extraordinary costs, our tax rate is the third lowest among OECD countries (only Turkey, Chile, and Mexico are lower).
Is it possible to indefinitely have high levels of health care spending, high levels of military spending, high incarceration rates and low taxes while still meeting the need for other public sector investments? Probably not. But clearly the argument that health care spending is responsible for the crowd out is at best overly simplistic.
At heart, if health care is expensive (which it is) and if income in our country is distributed very unequally (which it is), then making health care affordable for the average person will require substantial and growing transfer of wealth from the top to the bottom and even the middle. That is not ideology, that is math.
To some extent, the argument for reducing public health care spending is just budget austerity in a modified guise.
Myth: “It’s technological changes, stupid”
This one is also perhaps half true. Many leading health economists have attributed high rates of health spending growth to technology. But technology alone is not an adequate explanation. First, it doesn’t explain why technological change in health care seems to drive up spending while in other parts of the economy, technological advances often drive costs down. So there must be something specific about the interaction of technology and health care that drives spending up. Second, technological change per se is a very weak explainer of the difference in spending and spending growth between the US and other advanced industrial countries. Those countries all have access to the exact same technology. So it is there must be something specific about the way the US health care system combines with technology to lead to our particular pattern of cost growth. Also, technological change can be a major source of improved value in our system. Even if technology is a major driver of cost growth, we need to approach the issue carefully, focusing on weeding out the wasteful use of technology without impeding the development of medical advances.
Myth: “Not enough skin in the game”
Another explanation for our high levels of spending and spending growth is that people are “over-insured,” which insulates them from the cost of care and causes people to use more care than they otherwise would. As with technology, this explanation fails to account for the differences between the U.S. and other countries. Depending on how you measure it, out-of-pocket spending in the U.S. is either higher than other countries or more-or-less average. If lack of out-of-pocket spending were a driver of high health spending overall, then you would expect those countries with the lowest out-of-pocket spending to have the highest spending overall. But unlike per capita GDP, which correlates strongly with health spending, out-of-pocket spending levels have no strong correlation with total spending
Putting the cost debate in proper perspective
There is no obvious "right amount" to spend on health care.
It is pretty easy to calculate a level of health care spending that would align the U.S. with other industrial nations. There is a very strong correlation between per capita GDP and health spending.
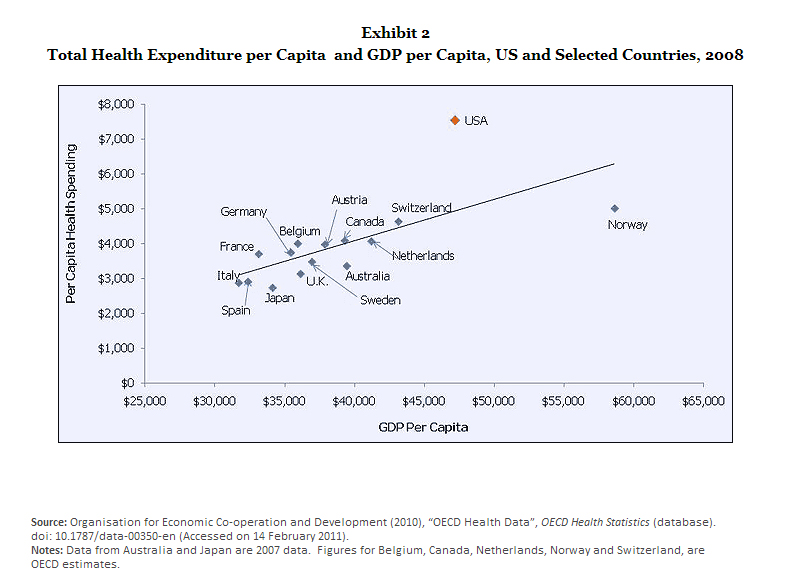
But there is nothing that really tells us that typical is the same as optimal. Americans have on average benefited greatly from increased health care spending. Bottom line: the “correct” level of health spending is unknown and probably unknowable.
So, does all that mean we don't really have a cost problem? Not exactly. While we don’t really know what we “should” spend, we do know that we don't seem to be getting nearly enough for the incremental increase in spending in the U.S. relative to other countries. Even though increased health spending over the past decades has brought many benefits, we could be benefitting just as much or more if we spent our health care dollars more efficiently and effectively. That’s why this blog series is titled Better Bang for the Buck. Focusing on cost alone rather than on value takes us off in the wrong direction. Reducing health spending is easy, at least conceptually if not politically. Reducing health spending while preserving or improving quality and access is where the hard work comes in. We’ll begin to build a framework for doing just that in a future blog.