This blog is part of a series that will highlight how structural racism in the health care system negatively affects the health of individuals of color. Community Catalyst is committed to exposing and dismantling policies, practices and attitudes that routinely produce cumulative and chronic adverse outcomes for people of color in the health system.
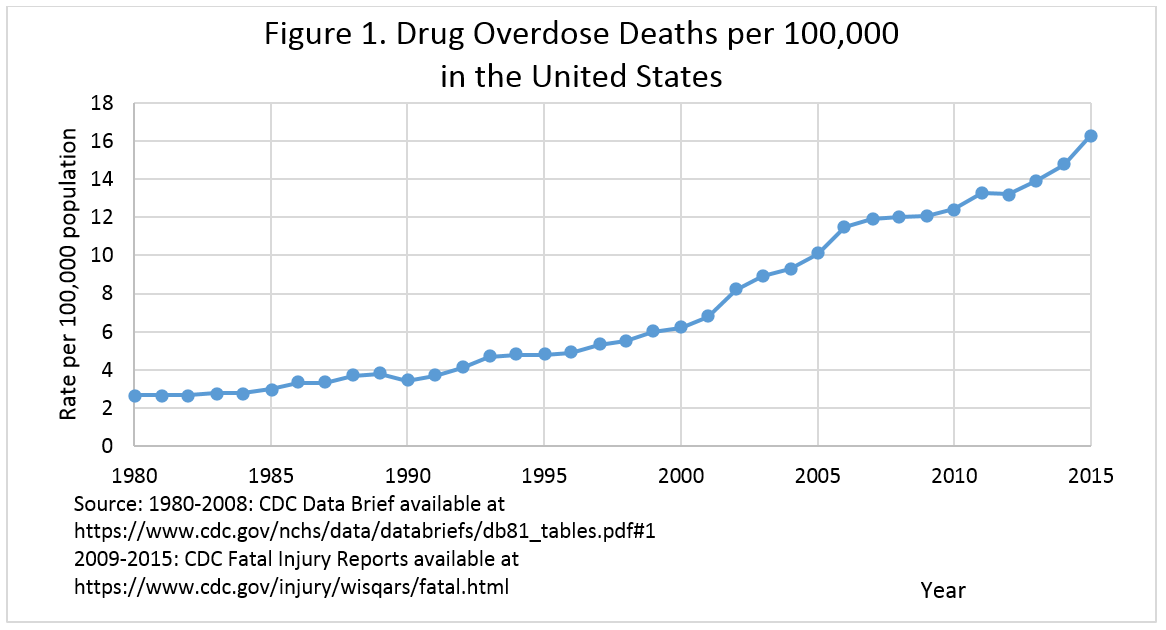
As health advocates work tirelessly to defend the Affordable Care Act in a wildly contentious partisan climate, we simultaneously find bipartisan efforts to combat the opioid crisis. But today’s overdose problem is not the first time our country has faced a devastating drug crisis—and even though drug overdose death rates now exceed those due to firearms and cars, overdose deaths have been increasing since 1980. So why the unified response now? Many outlets are rightly pointing out that the social and political reactions we see in the current opioid crisis differ dramatically from the criminalized approaches of the 1980s “War on Drugs.”
It’s important to look at how structural racism has contributed to the opioid crisis, and recognize that structural racism has also created the public motivation to try and do something about it.
What’s Different about the Opioid Crisis?
In short, the current opioid crisis has a different face.
The 1980s drug crisis was the “crack epidemic” and stereotypically portrayed as a phenomenon of “the violent black inner-city,” focusing on criminally dangerous drug addicts. Media coverage at the time shamed black mothers with addiction in particular, referencing “a time bomb in cocaine babies” and the “bio-underclass.” Crack was “reaching out to destroy the quality of life, and life itself, at all levels of American society.” In reality, the harm caused by the crack epidemic was not as severe as the media sensationalized. However, the resulting punitive approaches of the “War on Drugs” with harsh sentencing and mandatory minimums disproportionately affected communities of color with devastating effects.
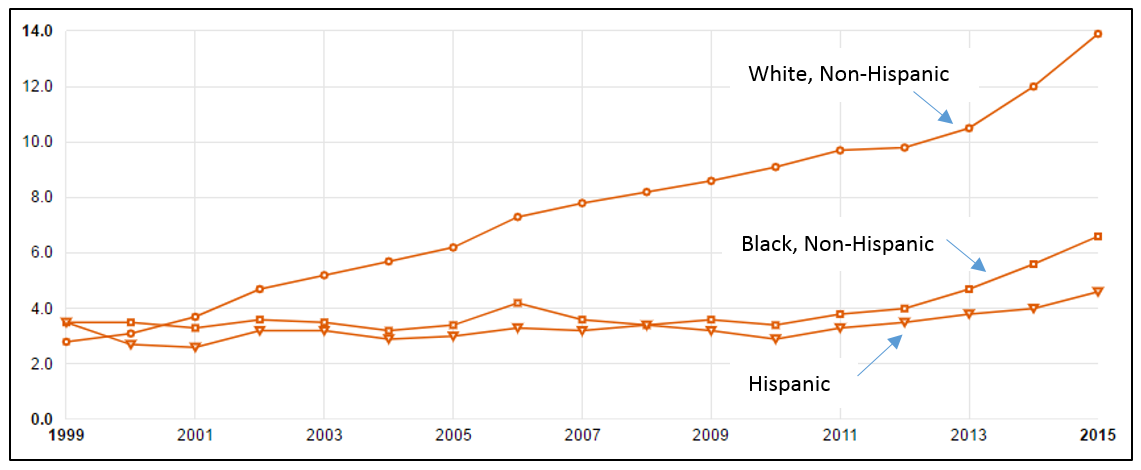
Today, we're shown a different face in the opioid crisis – a white one. Since 2001, the opioid overdose death rate among non-Hispanic whites has been higher than that of non-Hispanic blacks, and has sharply increased in recent years. With this new face comes a new response: rather than demonizing substance use as criminal behavior, our nation emphasizes treatment and public health interventions.
Opioid Overdose Deaths by Race/Ethnicity, Age-adjusted Rates Per 100,000 Population
Timeframe: 1999 – 2015
Source: Opioid Overdose Deaths by Race/Ethnicity, obtained from kff.org
Why is the opioid crisis disproportionately affecting whites?
Non-Hispanic whites make up more than 80-percent of opioid overdose deaths in the United States, and structural racism plays an important role in explaining this. A major driver of the current crisis is over-prescription of opioid pain relievers. Research shows communities of color have poorer health insurance coverage, less access to care, and get lower quality treatment than whites. Whites therefore may be more at risk of opioid overdose since they – and likely their family and friends – are more apt to be engaged in the health system to begin with, and thus more likely to obtain prescription pain medication.
On the whole, racist stereotypes lead to different pain treatments for black and white patients. Whether it’s the untrue assumptions that a black patient’s pain threshold is higher than their white counterpart or that a black patient is more likely to divert prescription pain pills to the illicit drug market, there’s a structural racism in the way pain is managed in this country.
How are the social and political responses different?
Studies show we are more likely to empathize with people who look like "us,” and policy-makers are more likely to be white. When law enforcement, elected officials and others in positions of power see themselves and their family members in opioid “victims,” they are more compelled to act with some compassion.
It’s why the punitive response to the crack epidemic has shifted to focus on treatment. Instead of criminals and selfish monsters, those misusing opioids are victims who need help.
One former narcotics officer described his new outlook:
“The way I look at addiction now is completely different…I can’t tell you what changed inside of me, but these are people and they have a purpose in life and we can’t as law enforcement look at them any other way…They need help.”
Substance use disorders have been affecting diverse communities for decades, but we are now focusing on the opioid crisis as a window of opportunity for shifting important public health policy. And in the words of Ekow Yankah, Law Professor at Yeshiva University:
“It is hard to describe the bittersweet sting that many African-Americans feel witnessing this national embrace of addicts. It is heartening to see the eclipse of the generations-long failed war on drugs. But black Americans are also knowingly weary and embittered by the absence of such enlightened thinking when those in our own families were similarly wounded. When the face of addiction had dark skin, this nation’s police did not see sons and daughters, sister and brothers. They saw “brothas,” young thugs to be locked up, rather than “people with a purpose in life.”
So, what do we do now?
We should not ignore the very real devastation of the current opioid crisis. Nor is the answer to structure health advocacy efforts solely on opioids, perpetuating the notion that because the problem has a “white face,” more people will care. That will only promote the structural racism we already see in our social, legal, political and health systems.
Instead, we need to employ a health equity approach by promoting policies that will equally benefit diverse populations: communities of color and white communities, rural and urban, young and old, wealthy and disadvantaged. We need to use a strategy that says “We don’t have to wait until a problem has a white face to answer with humanity.” This means calling out specific injustices when we encounter them, including Attorney General Jeff Sessions’ return to punitive policies for drug crimes. It also means building diverse coalitions to promote our policy issues.
Specific to substance use disorders policy, this also means advocating for treatment and prevention policies that refer to all substance use, and not opioids alone. To do anything else will continue to elevate the health of white people over communities of color.